

- Definition: OT helps children build the skills needed for daily life — dressing, writing, playing, and self-regulation.
- For Autism: Addresses sensory processing, social participation, fine motor skills, and independence.
- For ADHD: Targets executive function, attention, coordination, and emotional self-regulation.
- When to start: As early as possible — neuroplasticity is highest before age 5.
- What a session looks like: 45–60 minutes of structured, play-based 1-on-1 activities with a trained therapist.
- Key question to ask: Is the therapist RCI-registered with pediatric OT specialization?
Every parent who hears the words “your child might benefit from occupational therapy” goes through the same sequence: relief that there is help, then confusion about what that help actually means. The word “occupational” sounds like it belongs in an office, not a child’s therapy room. And most articles that try to explain OT are written for clinical professionals, not for a mother in Patna trying to decide whether to book that first appointment.
This guide is for that mother — and that father, that grandparent, that teacher. It explains exactly what occupational therapy is, what your child will actually do in a session, why the research on early intervention is so compelling, and what separates a truly effective OT center from one that produces slow, inconsistent results. By the end, you will have the knowledge to make a confident, informed decision for your child.

What Is Occupational Therapy? (And Why the Name Is Misleading)
The word “occupational” does not refer to a job or a career. In therapy, it refers to every meaningful activity that occupies a person’s time — and for a child, that means playing, eating, dressing, writing, making friends, and learning. Occupational therapy (OT) is a health profession that helps people of all ages develop, recover, or maintain the daily skills that make independent life possible.
For children with Autism and ADHD, the daily skills that need building are often invisible to untrained eyes: the ability to sit without sensory discomfort, to hold a pencil without frustration, to tolerate a birthday party without a meltdown, to make eye contact during conversation. These are not small things. They are the building blocks of a child’s entire social and academic life.
In India, occupational therapists must be registered with the Rehabilitation Council of India (RCI) and hold at minimum a Bachelor of Occupational Therapy (BOT) degree from a recognized institution. Therapists with a Master of Occupational Therapy (MOT) and additional pediatric specialization — particularly in sensory integration — are equipped for the most complex neurodevelopmental cases. Occupational therapy is recognized and recommended for Autism treatment by the American Academy of Pediatrics (AAP), WHO, and India’s own National Trust guidelines.
Key Distinction: OT is often confused with physiotherapy (PT) and speech therapy. PT focuses on gross motor movement and physical rehabilitation. Speech therapy addresses communication and language. OT sits in the middle — it works on the functional, daily-life application of motor, cognitive, and sensory skills. Many children need all three, which is why a center offering them under one roof matters enormously.
How Occupational Therapy Helps Children with Autism
Autism Spectrum Disorder (ASD) affects children differently — some are highly verbal, some nonverbal; some are hypersensitive to sound, others seek intense sensory input. What nearly all children with Autism share is that certain everyday tasks — tasks most children learn automatically — require deliberate, structured support to develop. Occupational therapy provides exactly that structure.
The 5 Core Areas OT Targets in Children with Autism
| OT Focus Area | What It Means for Your Child | Example Goal |
|---|---|---|
| Sensory Processing | Learning to tolerate and enjoy sensory experiences — touch, sound, movement | Tolerates wearing clothes without distress; sits in a noisy classroom |
| Fine Motor Skills | Small muscle coordination for writing, buttoning, using cutlery | Holds pencil correctly; writes name legibly |
| Social Participation | Play skills, turn-taking, eye contact, understanding social cues | Engages in 5-minute cooperative play with a peer |
| Self-Care Independence | Dressing, grooming, eating — performing these without distress or adult help | Dresses independently in the morning routine |
| Emotional Regulation | Recognizing and managing emotions, reducing meltdown frequency and intensity | Uses 3 self-calming strategies when overwhelmed |
📚 Research — 2024
A 2024 study published in Cureus (PubMed ID: 39109123) evaluated OT outcomes in 40 children with ASD aged 3–9 using the Autism Behavior Checklist. It found significant, measurable improvements across sensory skills, language development, relationship-building abilities, and self-care competencies following sensory integration-based occupational therapy. The authors concluded that OT should be a first-line intervention rather than a supplementary one for children with Autism.
📖 Real-World Example
Riya, aged 4, Patna: Riya refused to eat anything with texture — her diet had narrowed to three foods, and mealtimes had become a daily crisis. After 12 weeks of occupational therapy targeting oral sensory processing and feeding skills, Riya’s food tolerance expanded to 11 foods. Her mother described the shift as “getting our family back.” This is the kind of outcome that a well-run Autism Treatment Center in Boring Road, Patna works toward — not just clinical milestones, but real daily life change.
How Occupational Therapy Helps Children with ADHD
Attention-Deficit/Hyperactivity Disorder presents differently from Autism — but the overlap in OT treatment areas is significant. Children with ADHD often struggle not because they cannot understand a task, but because their brain’s executive function system — the internal manager responsible for planning, initiating, and following through on tasks — does not work the way neurotypical brains do. Occupational therapy for ADHD focuses specifically on building these executive skills alongside managing the sensory factors that amplify inattention.
A March 2024 study in Research in Developmental Disabilities confirmed that atypical sensory processing is significantly more prevalent in adolescents with ADHD than in neurotypical peers, validating the sensory integration approach in OT for ADHD. This means the same sensory tools that help Autism — weighted lap pads, movement breaks, fidget tools, and structured sensory diets — are directly applicable and effective for ADHD.
One of the most valuable but least-discussed benefits of OT for ADHD is its work on Developmental Coordination Disorder (DCD) — a condition where motor planning and coordination are impaired. Research shows DCD co-occurs in approximately 50% of children with ADHD, yet it is rarely identified without a formal OT assessment. Children who struggle with handwriting, PE class, or tying shoelaces may have DCD, not just ADHD inattention — and OT directly treats it.
The Zones of Regulation — OT’s Framework for ADHD Self-Control
One of the most evidence-backed tools occupational therapists use with ADHD children is the Zones of Regulation framework — a system that teaches children to categorize their emotional state into four colored zones and identify strategies to move between them. Children as young as 5 can learn to recognize when they are in the “Red Zone” (furious, out of control) vs. the “Blue Zone” (low energy, sad) and apply the right coping strategy. This skill alone dramatically reduces classroom disruptions and homework battles.
📖 Real-World Example
Arjun, aged 7, Boring Road area: Arjun’s teachers reported he couldn’t complete a single homework task without a meltdown. His mother assumed it was behavioral. An OT assessment revealed he had significant sensory sensitivity to background noise, poor proprioceptive processing, and difficulty initiating tasks — all treatable OT targets. After 16 weeks combining sensory diet planning and executive function coaching, Arjun completed homework independently for the first time. His teacher’s exact words: “He’s a different child.”
What Happens in a Child’s Occupational Therapy Session? (Step by Step)
One of the most common worries parents bring to a first appointment is: “My child won’t cooperate — they hate new places and new people.” This is a valid concern, and a good OT therapist is specifically trained to address it. Here is exactly what a well-structured OT session looks like at a specialist pediatric center.
- Initial Assessment (First Visit — 60–90 min): A certified therapist conducts standardized evaluations — such as the Sensory Processing Measure (SPM) or Peabody Developmental Motor Scales — combined with a detailed parent interview and structured observation of the child at play. No treatment begins without this baseline.
- Goal Setting (With You, Not Just for You): Therapist and parent co-create 3–5 specific, measurable goals. Not vague targets like “improve social skills,” but concrete milestones: “Will independently button shirt within 8 weeks” or “Will tolerate 15 minutes in a noisy environment by Session 12.”
- Active Therapy Session (45–60 min, 1-on-1): Your child works one-on-one with their dedicated therapist using play-based activities, sensory equipment (therapy swings, tactile bins, balance boards, crash mats), fine motor tasks, and structured social play. Sessions feel like play — they are designed to. The learning is embedded in the activity.
- Parent Coaching (Last 10 Minutes): The therapist demonstrates 2–3 home activities and explains why each one targets your child’s specific goals. This ensures progress continues between sessions. Parent involvement at this stage consistently doubles the rate at which children generalize new skills to real life.
- Monthly Progress Review: Written progress report comparing current performance against baseline goals. Goals are updated, advanced, or modified based on evidence of improvement. Parents receive a clear picture of where their child stands and what comes next.
Why the 1-Child : 1-Therapist Ratio Is Non-Negotiable
Children with Autism and ADHD process information differently and need predictable, undivided therapeutic attention. A therapist managing 3 or 4 children simultaneously cannot track the micro-signals — a flinch at a texture, a moment of eye contact, a shift in arousal level — that guide effective OT. One child, one therapist, every session is not a luxury. It is how real progress happens.
The 8 Sensory Systems: What Most Parents (and Many Clinics) Don’t Know
When people discuss sensory issues, they typically mention the five senses — sight, hearing, touch, smell, and taste. But children with Autism and ADHD are most affected by three additional sensory systems that most parents, and even some clinics, rarely mention. Understanding all eight is essential to understanding why your child behaves the way they do in certain environments.
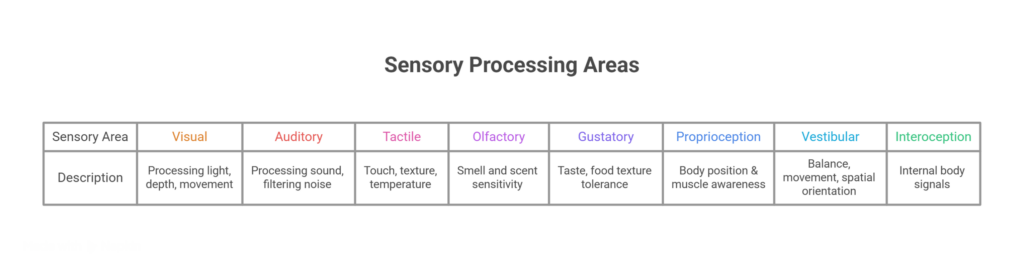
The three highlighted systems — proprioception, vestibular, and interoception — are the ones most implicated in Autism and ADHD meltdowns, sensory-seeking behaviors, and emotional regulation difficulties. A child who constantly crashes into furniture is seeking proprioceptive input. A child who spins in circles is self-regulating their vestibular system. A child who cannot identify when they are hungry or anxious has interoceptive processing differences. Sensory Integration (SI) therapy, developed by Dr. A. Jean Ayres, directly addresses these systems through structured, play-based activities using specialized equipment.
📚 Research — 2025
A 2025 systematic review and meta-analysis published in Frontiers in Psychiatry examined the effectiveness of Sensory Integration-based interventions in autistic children, with data synthesized from multiple randomized controlled trials. The review confirmed statistically significant improvements in sensory processing, adaptive behavior, and daily living skills in children who received structured SI therapy compared to control groups. The authors specifically recommended SI as a core component of Autism OT programs — not an optional add-on.
Why Occupational Therapy and Speech Therapy Together Produce Better Results
A 2024 meta-analysis published in Pediatrics, covering 22 studies and thousands of children, found that children with Autism who received combined occupational therapy and speech therapy interventions showed 2.3 times greater gains in functional communication and daily living skills compared to those receiving only one type of therapy. The reason is straightforward: Autism and ADHD affect multiple systems simultaneously, and treating only one system while leaving others unaddressed is like fixing one broken wheel on a car and wondering why it still veers off course.
For children in Patna seeking comprehensive neurodevelopmental support, this means the location and structure of the therapy center matters as much as the quality of individual therapists. When an occupational therapist and a speech therapist work in different clinics, they rarely communicate. Goals get set in isolation. The OT works on a child’s ability to sit and focus — but the speech therapist, unaware of this work, runs sessions that inadvertently undermine the OT’s sensory regulation plan. This fragmentation is the silent reason many children plateau despite months of therapy.
Families searching for a Speech Therapy center in Boring Road, Patna that also provides occupational therapy in the same facility benefit from a unified team approach — where both therapists read the same assessment, share the same goal sheet, and adapt their individual plans in coordination.
When Should You Start OT? The “Wait and See” Myth — Addressed Directly
In Bihar, and across much of India, parents of children showing developmental differences are frequently advised by well-meaning family members, and occasionally by general practitioners unfamiliar with early intervention, to “wait and see if they grow out of it.” This advice, though offered with care, is one of the most damaging patterns in pediatric neurodevelopmental care.
The science on neuroplasticity is unambiguous: the brain’s capacity for structural reorganization — its ability to form new neural pathways in response to therapy — is significantly higher in the first five years of life than at any subsequent period. Children who receive OT intervention between ages 2 and 5 show meaningfully better long-term outcomes in communication, social participation, academic readiness, and daily independence than children whose therapy begins at age 7, 8, or later. Waiting does not give the brain time to “catch up.” It costs time that cannot be recovered.
| Age Group | Key OT Focus Areas | Signs to Watch For |
|---|---|---|
| Toddlers (18 months – 3 yrs) | Sensory tolerance, play exploration, feeding, early motor skills | Extreme food refusal, avoids being touched, delayed walking or grasping |
| Preschool (3 – 5 yrs) | Sensory regulation, peer play, pre-writing skills, self-care | Meltdowns at transitions, avoids playgrounds, cannot hold crayon |
| School-Age (6 – 12 yrs) | Handwriting, classroom focus, social skills, homework routines | Illegible writing, can’t sit through class, avoids group activities |
| Teens (13 – 18 yrs) | Executive function, independence skills, vocational readiness | Cannot manage schedule independently, struggles with transitions to new environments |
Important: You Do Not Need a Diagnosis to Book an Assessment: Many parents wait until they have a formal Autism or ADHD diagnosis before seeking OT — sometimes taking months or years navigating the diagnostic pathway. An experienced Autism Doctor in Boring Road, Patna can begin the assessment and therapy process based on observed developmental patterns, even before a formal diagnosis is confirmed. Early functional intervention is not contingent on a diagnostic label — it is a response to a child’s actual, observable needs.
How to Choose the Right OT Center in Patna — A Parent’s Checklist (and Red Flags)
Not all therapy centers are equal, and in a city like Patna, where awareness of occupational therapy is still growing, parents can find it difficult to evaluate the quality of a center before committing. The following two lists — green flags to look for and red flags to walk away from — will help you make a confident, informed choice.
✅ What a Good OT Center Looks Like
- Therapists hold BOT or MOT degrees with valid RCI (Rehabilitation Council of India) registration
- Formal assessment is conducted before therapy begins — not after the first session
- Strict 1-child : 1-therapist ratio for every session
- Therapist has specific training in sensory integration (Ayres SI or equivalent)
- Written therapy goals are shared with parents at the outset
- Monthly progress reports with measurable outcomes, not vague verbal updates
- Parent coaching is built into every session — not occasional
- Multiple therapies available under one roof (OT + Speech + Behavior)
- Child-friendly, sensory-thoughtful environment — calm, structured, consistent
- Location is accessible — consistent attendance directly predicts outcomes
🚫 Red Flags — Walk Away If You See These
- Therapy begins without any formal assessment or parent interview
- One therapist is managing 3 or more children at once
- No written goals provided — just verbal assurances
- No parent involvement in sessions or at-home guidance
- Progress updates are vague (“doing better”) with no measurable data
- Therapist cannot explain their qualifications or RCI registration number
- Session environment is loud, chaotic, or unstimulating
📖 Real-World Example
Priya, aged 3, single mother from Patna: Priya’s mother initially enrolled her at a nearby center that offered “OT and speech” but only had one general therapist managing four children simultaneously. After two months with no visible progress and no written reports, she switched to a dedicated Occupational Therapy center in Boring Road, Patna with a strict 1:1 model and structured parent coaching. Within six weeks of consistent 1:1 sessions, Priya’s therapist documented the first measurable improvements in sensory tolerance and fine motor control.
What to Bring to Your Child’s First OT Assessment
This section exists nowhere on competitor websites — but parents search for it constantly. Walking into your child’s first OT assessment well-prepared makes the session more productive and gets you to a meaningful therapy plan faster. Bring the following:
- Any previous diagnostic reports (Autism, ADHD, developmental delay assessments)
- School report cards or teacher observations about behavior and performance
- A short video on your phone of concerning behaviors at home — meltdowns, sensory reactions, feeding difficulties. Therapists cannot observe these in a clinic setting, and a video is worth more than a description
- A written list of your top 5 concerns in order of priority — this ensures the therapist focuses on what matters most to your family
- Your child’s current daily routine (wake-up, meals, school, bedtime) — this context shapes how goals are set
- Any food allergies or sensory triggers your child has shown to specific textures, sounds, or lighting
Conclusion
Occupational therapy is not a supplementary treatment or a last resort. For children with Autism, ADHD, or other neurodevelopmental differences, it is one of the most evidence-backed, life-changing interventions available — one that addresses the daily skills that determine whether a child can dress themselves, sit through school, make a friend, and eventually live with independence and confidence.
The quality of the center where your child receives OT will determine how fast and how far they progress. You now have the knowledge to evaluate that quality: the right qualifications to ask for, the right process to expect, the sensory systems that matter most, and the red flags that should send you elsewhere.
At Rehab for Autism & ADHD — a specialized Autism Treatment Center in Boring Road, Patna — every element of this guide is not just a recommendation but our everyday practice. Led by Dr. Kapil Dev (BOT, MOT, ex-Senior Consultant Occupational Therapist at AIIMS Patna) and a team of RCI-registered pediatric specialists, we offer Occupational Therapy, Speech Therapy, Sensory Integration, Behavior Therapy, and Special Education — all under one roof, all on a strict 1-child : 1-therapist basis, all guided by formal assessments and measurable goals. Our center at C17, Sri Krishna Puri, Patna, Bihar 800001 is built for one purpose: to give every child who walks through our doors the most effective, most personalized therapy available in Bihar.
Accessibility from Across Patna
Our centre at C17, Sri Krishna Puri is easily reachable from across central Patna. Families regularly visit from near Bihar Museum (900 m, 3 mins), Eco Park (1.9 km, 6 mins), Patna Museum (2.5 km, 8 mins), ISKCON Temple Patna (2.6 km, 7 mins), and Buddha Smriti Park (3.0 km, 10 mins). Families from the Sanjay Gandhi Biological Park (3.5 km, 9 mins) area, near Golghar (3.7 km, 14 mins), and P&M Mall (4.7 km, 16 mins) all reach us conveniently. Nearby landmarks: A.N. College (1.6 km), Jyoti Punj Hospital (1.1 km), GV Mall near Boring Rd (1.3 km), Panchmukhi Hanuman Mandir (1.8 km). Consistent attendance is one of the most powerful factors in therapy progress. Choosing a centre close to home removes one of the biggest barriers to regular sessions.
Ready to Take the First Step?
Book a detailed assessment at Patna’s specialist Autism, ADHD & Occupational Therapy center on Boring Road. Our team will evaluate your child’s needs, explain your options clearly, and build a therapy plan designed specifically for your child — not a template.
📅 Book an Appointment: https://rehabautismadhd.org/book-appointment/
💬 Mail us : Rehabforautismandadhd2019@gmail.com
info@rehabautismadhd.org
Mon – Sat · 12:00 PM – 8:00 PM · C17, Sri Krishna Puri, Patna, Bihar 800001
Frequently Asked Questions About Occupational Therapy
Q. What is the difference between occupational therapy and physiotherapy?
A. Physiotherapy (PT) focuses primarily on gross motor movement, physical rehabilitation after injury, and musculoskeletal conditions. Occupational therapy (OT) focuses on the functional skills needed for daily life — sensory processing, fine motor coordination, self-care, social participation, and cognitive organization. While PT asks “can this child walk?”, OT asks “can this child dress themselves, write legibly, and sit in a classroom without distress?” Both are valuable, and many children benefit from both.
Q. How many OT sessions does my child need before seeing results?
A. This varies based on the child’s age, the severity of challenges, the frequency of sessions, and the degree of parent involvement between appointments. Many parents notice meaningful behavioral changes within 6–8 weeks of consistent, 1-on-1 OT. Measurable progress against formal goals typically shows within 3 months. Children who practice home activities between sessions consistently progress faster than those who only attend clinic sessions.
Q. What is a sensory diet and how does it help a child with ADHD?
A. A sensory diet is a customized daily schedule of sensory activities — designed by the OT therapist specifically for your child — that provides the right type and amount of sensory input throughout the day to keep their nervous system regulated. For ADHD, this might mean a 5-minute “heavy work” activity (pushing a loaded cart, carrying books) before sitting down for homework, or scheduled movement breaks every 20 minutes during study time. A well-crafted sensory diet reduces meltdowns, improves attention, and makes academic tasks more accessible.
Q. Can occupational therapy cure Autism?
A. No — and any therapist or center claiming a “cure” for Autism should be approached with caution. Autism is a neurodevelopmental difference, not a disease. Occupational therapy does not change who a child is. What it does is build the functional skills that allow a child to participate more fully and comfortably in daily life — reducing the impact of sensory differences, building independence, and improving quality of life for both the child and their family. These are meaningful, real outcomes that evidence consistently supports.
Q. Does occupational therapy help with handwriting problems?
A. Yes — improving handwriting is one of the most common goals in pediatric OT referrals. Poor handwriting is usually a symptom of underlying fine motor skill deficits, poor pencil grip, low muscle tone, or visual-motor integration difficulties — all of which OT directly addresses. Rather than drilling letter formation (which doesn’t fix the underlying problem), OT therapists use activities that build the foundational skills that make legible handwriting possible.
Q. Do I need a formal Autism or ADHD diagnosis before booking an OT assessment?
A. No. At our center, an OT assessment can be booked based on observed developmental concerns — even if your child has not yet received a formal diagnosis. Early functional assessment and intervention is not contingent on a diagnostic label. If you notice your child is struggling with sensory experiences, daily routines, motor skills, or social interaction, an assessment is the right next step, regardless of whether a formal diagnosis has been given.
Q. How is OT different when a child has both Autism and ADHD?
A. Co-occurring Autism and ADHD — which research suggests affects approximately 50–70% of individuals diagnosed with one of the two conditions — requires a carefully integrated OT approach. The therapist must balance sensory regulation work (more central to Autism) with executive function development (more central to ADHD), while ensuring that strategies used for one do not conflict with the other. This is exactly why assessment before therapy is non-negotiable, and why experienced pediatric OT specialists with multi-condition expertise produce better outcomes.
Q. What is the cost of occupational therapy in Patna?
A. OT session costs in Patna vary based on the therapist’s qualification level, whether sessions are individual or group, and the center’s infrastructure. At a specialist pediatric center with RCI-registered therapists, structured 1:1 sessions, sensory integration equipment, and formal progress reporting, costs reflect the clinical quality being delivered. We encourage parents to evaluate OT cost against the value of consistent, measurable progress — and to ask any center directly about their session structure, therapist qualifications, and goal-setting process before making a decision based on price alone. Contact us for current session information.




